For the last 7 months, I’ve had the pleasure of working alongside our next guest contributor to the blog, Chee Vang, PT, DPT, CSCS, USAW, CCWC (a.k.a., alphabet soup!). Chee is one of our current ortho PT residents. Please enjoy his piece on squat mechanics and variations, and please feel free to engage with him and others via comments and discussion below. Enjoy!
The Squat
The squat is one of the most versatile exercises performed in rehabilitation and in athletics to enhance lower extremity strength. This is a movement pattern that I have spent countless hours trying to master in my practice of Olympic weightlifting. When training my athletes, I continually promote the squatting pattern with the well-known “ass to grass” model in their position of comfort/position of strength, but in my clinical practice I’ve been more conscious as to the specific form of the squat being performed. The squat is not only utilized to enhance athletic performance, but is as versatile a movement for the non-athletic population. Picture a 21-month-old squatting to play with a toy on the floor compared to an older individual lowering their body to a chair – probably a different squat form, right? So, what is the optimal squat form? Below I will highlight different components to the squat that I believe should be considered with squat prescription and provide information to help answer (1) What type of squat should be performed? (2) How deep should we squat? (3) Can the knees pass the toes? and (4) Should the stance be narrow or wide?
What type of squat should be performed?
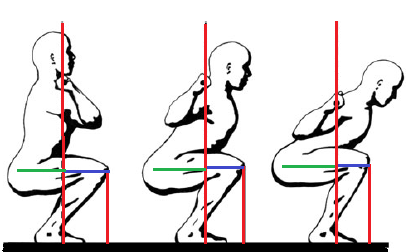
(A) (B) (C)
The common squatting techniques that can be performed include the front squat and back squat.1 There are many variations that can be progressed/regressed based on these two forms of squats.
The front squat (A) allows for a more upright trunk position with increased anterior knee excursion and demonstrates increase moment arm in the knee joint (relative to the lowest positions, keeping in mind that the squat is a dynamic movement and these moment arms change through the squat). This increased moment arm will increase the demands of the quadriceps, compared to the back squat. The front squat variation is not as commonly performed in the rehabilitation setting, with most clinicians having an increased focus on performing the “glute dominant” back squat.
The back squat includes the high bar (B) and low bar (C) squats. Both back squat positions demonstrate an increase forward trunk lean with less anterior knee excursion compared to the front squat along with a more vertical tibia/fibula and demonstrates increased moment arm in the hip joint, increasing the demands of the hip musculature. The low bar promotes a greater forward trunk lean. This position also reduces patellofemoral compression and ACL strain compared to front squats. This more closely mimics the “glute dominant” squat that is more commonly instructed in rehabilitation settings. Keep in mind, the images below are demonstrating positioning with a barbell. Many times, in rehabilitation, external load may not initially be added to a squat. However, should we always consider adding external weight to allow for progressive overload if our goal is to strengthen? (This is a topic for another time!).
The front squat may be beneficial to implement when trying to bias more quadriceps activity, although the back squat/“glute dominant” squat will provide increase hip/gluteal demands which is a common goal in rehabilitation. We often promote a glute dominant squat because many individuals we help rehabilitate lack hip strength and muscular control required for functional activities. However, we may be missing out on the use of a front squat for individuals who may require more emphasis on strengthening their quadriceps.
How deep should we squat?
There are varying depths to which a squat can be performed from a partial squat (knee flexion angle of about 40°), half squat (knee flexion angle of 70 to 100°), and a deep squat (knee flexion angle greater than 100°). When no known pathology is present in the hips, knees, or ankles/foot, I believe we should squat to our full available range of motion. Consider some of these findings:1-2
- 90° is where the greatest retropatellar forces occur.
- This is where many individuals may stop when performing the squat, which is less likely recommended for individuals with patellofemoral pain.
- Increased compressive forces at the knee occur during deeper squats especially at deep knee flexion angles, along with greater stress for the menisci and articular cartilage.
- The ACL and PCL are mostly affected by shear forces.
- Anterior shear is controlled by the ACL which peaks in the first 30° of knee flexion and it is suggested that by about 60° of flexion, the anterior shear force is decreased.
- Posterior shear begins at about 30° of knee flexion but peaks at about 90° of flexion. Posterior shear forces are suggested to decrease beyond 90°, which is again suggested due to the approximation of soft tissue.
- Schoenfeld et al (2010) suggests individuals with existing knee injury or previous PCL reconstruction may only need to squat to 50-60° of flexion to minimize posterior shear forces.2
- Deep squats show forces generated in the knee are “shared and dispersed” due to soft tissue approximation of the gastrocnemius and distal hamstrings.
- For individuals with intact ACL and PCL, the shear forces during deep squats are not typically enough to damage the ligaments (though this does not mean that it cannot happen).
- Quadriceps muscle activity does not appear to increase beyond the parallel squat.
- Average muscle activity of the gluteus maximus was not significantly different in a partial squat compared to a parallel/half squat, but it did increase significantly with a deep squat.
To summarize this literature, we should consider the individual’s specific activity/sport demands when considering squat depth. An individual without any pathology in the hip/knee/ankle may benefit from squatting through their full available motion, but this may exacerbate the symptoms for individuals with patellofemoral dysfunction, cartilage compromise, or hip/ankle impingement.
Can the knees pass the toes?
In 2003, Fry et al studied two types of squats, a restricted versus an unrestricted squat.3 The restricted squat had a board placed in front of the toes which prevented anterior knee excursion beyond the board/foot (closely mimicking picture C from above) while the unrestricted squat allowed for some anterior knee excursion beyond the toes (picture A). The intensity and volume of squats was comparable between the two groups.
Fry et al found that the unrestricted squat demonstrated a 28% increase in torque at the knee joint compared to the restricted squat. Fry also found close to a 1000% increase in torque at the hip for the restricted squat compared to the unrestricted squat, increasing the demands at the hip. Trunk inclination angle was greater with a restricted squat, which also suggested an increase of shear forces to the lumbar spine compared to the unrestricted squat.
The restricted squat again mimics the position that many rehabilitation specialists will begin with, and we often cue patients to avoid anterior knee excursion. For individuals with lumbar spine pathology that we instruct in performing the squat pattern, we often cue for a hip hinge and to minimize anterior knee excursion. If an individual does not have any hip or lumbar pathologies, they may respond well to the restricted squat. The unrestricted squat will allow for an increase in anterior knee excursion, but may demonstrate less shear forces across the lumbar spine.
Should the stance be narrow or wide?
In 2009, Paoli et al assessed electromyographical (EMG) activity of eight thigh muscles in six individuals using no external load, 30% of 1 Repetition Max (RM), and 70% of 1 RM at three different stance widths during the back squat.4
They found as external load increased from none to 70% of 1 RM, all muscles EMG activity increased (of course, we all know that increasing load will have this effect). Gluteus maximus activation increased with no external load and at 70% 1 RM as the squat width increased, but the other seven muscles did not demonstrate a statistically significant improvement in EMG activation in response to increasing squat width.
Schoenfeld (2010) also reported:2
- 15 % increase in patellofemoral and 16% increase in tibiofemoral compressive forces in individuals utilizing a wider squat stance compared to a narrower stance.
- Narrow stance resulted in 4 to 6 cm greater anterior knee excursion, suggesting increased shear forces at the knee.
- Gastrocnemius activity increases up to 21% with a narrow stance compared to a wide stance.
Besides power lifters, a wide stance has minimal specificity to daily tasks but does not mean it does not have its place. A wide stance can be a pattern performed as an accessory movement to maximize gluteus maximus activation, however, this can be met with increasing external load.
Take Home Points:
Consider the individual, specific tasks, and environmental factors as these are important to determine squat prescription prior to labelling dichotomies for “the optimal squat.”
Front Squat versus Back Squat:
The back squat/“glute dominant” squat will increase the demands of the hip musculature, along with minimizing patellofemoral compression and ACL strain, while the front squat may be advantageous for increasing quadriceps activity.
Depth:
Partial and half squats will provide less strain to the ligamentous tissue in the knee and less patellofemoral compression, while deeper squats may be advantageous to increase gluteal activation.
Anterior Knee Excursion:
Some anterior knee excursion allows for a more upright trunk position, inducing less torque at the hip and shear forces at the lumbar spine, but shows an increase in torque at the knee joint.
Stance:
Wide squat stance can facilitate gluteus maximus activation, however, also appears to increase compressive forces at the knee joint.
References:
- Hartman H, Wirth K, Klusemann M. Analysis of the load on the knee joint and vertebral column with changes in squat depth and weight load. Sports Med. 2013;43:993-1008.
- Schoenfeld BJ. Squatting kinematics and kinetics and their application to exercise performance. J Strength Cond Res. 2010;24(12):3497-3506.
- Fry AC, Smith JC, & Schilling BK. Effect of knee position on hip and knee torques during the barbell squat. J Strength Cond Res. 2003;17(4):629-633.
- Paoli A, Marcolin G, & Petrone N. The effect of stance width on the electromyographical activity of eight superficial thigh muscles during back squat with different bar loads. J Strength Cond Res. 2009;23(1)246-250.

Hugo- just catching up on emails. Thanks for your work and summary on this. It’s great to have a structured breakdown of the how and why to select the various approaches to this exercise. The one size fits all approach to squats clearly leaves room for improvements, and these points can efficiently help steer clinicians to match the right approach to the right patients.
Thanks again!
LikeLike